Primary (or focal) hyperhidrosis most commonly affects hands (palmar hyperhidrosis), feet (plantar hyperhidrosis) and underarms (axillae), but can also affect the face and head or other areas including the back, neck, groin, legs and buttocks. It affects both sides of the body equally, and often starts in adolescence or even childhood. Typically, it is not present when asleep, and it can run in families. The cause is not known, although anxiety can make it worse. Although it is not temporary, it can sometimes improve with age. Approximately half a million people in the UK are affected.
Secondary hyperhidrosis can affect the whole body (generalised hyperhidrosis) or specific areas, or it may only affect one side of the body. People with secondary hyperhidrosis often sweat while asleep. It can be caused by illness or infection, obesity, or hormonal conditions such as an over-active thyroid, the menopause or diabetes. Localised secondary hyperhidrosis can occur as a result of trauma or following surgery to the chest. It can also be a side effect of certain medications, including SSRI anti-depressants such as fluoxetine (Prozac). These causes must be ruled out before primary hyperhidrosis can be diagnosed.
CAUSES
While doctors don't know why primary hyperhidrosis starts, they have successfully linked it to over-activity in the sympathetic nervous system. Specifically, it is the Thoracic Sympathetic Ganglion Chain, which runs along the vertebra of the spine inside the chest cavity.
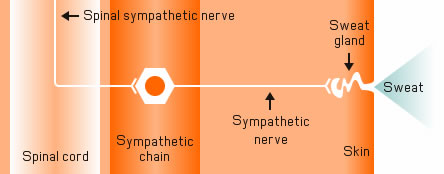
Diagram courtesy of Mr Mark Whiteley
This chain controls the glands, known as the apocrine and eccrine glands, responsible for perspiration throughout the entire body. Depending on which part of the chain becomes overactive, different parts of the body become affected.
To find out more about some of the affected areas, please follow the links below to the appropriate page
Find out more about how hyperhidrosis affects different sites: